Podcast
Dr. Ganzevoort, expert-by-experience Alberdien Kenbeek (volunteer at Care4Neo), and midwife Joyce Schouten explore the clinical and emotional journey of FGR, covering topics from the initial diagnosis through pregnancy, birth, and the long-term impact that follows.
In this conversation, they address questions such as: What does the diagnostic and management process for FGR entail? How does this diagnosis and the subsequent trajectory impact the emotional and physical wellbeing of the woman, her partner, and her social environment? The podcast offers invaluable insights from a diverse range of perspectives – patients, partners, and healthcare professionals. A bit of a long listen, but worth the time!
What is fetal growth restriction (FGR)?
Fetal growth restriction is the condition when a baby does not grow in the womb as expected. The most common cause is that the placenta that does not provide enough nutrients and oxygen to the baby. This can cause serious health problems, especially early in the pregnancy. FGR is typically diagnosed by growth ultrasounds and other tests. It is important to know that most cases of FGR are carefully monitored to ensure the best outcomes for both mother and baby.
What is the function of the placenta?
The placenta is attached to the womb and the umbilical cord connects the baby to the placenta. In the placenta, the blood of the mother and the baby flows very close to each other. This allows the transport of nutrients and oxygen towards the baby and waste products towards the mother. A good exchange between baby and mother is needed for the baby to grow properly during pregnancy. If the placenta does not work well, the baby cannot grow properly and – as an end-stage consequence – can be damaged by low oxygen levels.

What is normal fetal growth and how is this determined?
Each baby has its own growth pattern. Just like in adult life, there is natural variation, especially in the later phases of pregnancy. Around 20 weeks of pregnancy, the average baby weighs about 300 grams, increasing to about 1200 by 28 weeks and about 1900 grams at 32 weeks. In these 4 weeks only, babies grow nearly 60% on average! After 32 weeks, the growth rate gradually slows down.
In pregnancy, we compare the size of a baby with normal values using percentiles. This means we look at the baby’s measurements and compare them to those of other babies at the same gestational age of pregnancy. This is often displayed in a growth curve (like the example below). For example, if a baby is at the 40th percentile (p40), this means that approximately 40% of babies at that gestational age are smaller, and 60% are larger. If the baby is around the same percentile in later measurements (following its own line), growth is assumed to be normal for this baby.
Read more
One way to estimate the baby’s size is by assessing the fundal height of the womb. Here, your care provider feels the top of the womb through the abdomen and compares it to a standard for that gestational age. If this seems to be abnormal, or if it is challenging to feel in case of obesity, or if there is an increased risk of FGR, a growth ultrasound is typically recommended. During this ultrasound, measurements of the head, abdomen, and femur are taken and combined to estimate the weight of the baby (estimated fetal weight). It is important to note that these measurements are also not extremely precise, so that this number should be interpreted as an estimation rather than a scale weight. The actual weight can sometimes be 10% more or less than the estimated fetal weight.
Also, with one measurement we know the baby’s size, as a reflection of past growth. With repeated ultrasound measurements, caregivers can get an estimation of current growth. To accurately assess growth, these measurements are usually done at least 14 days apart. This interval makes sure that the measurement uncertainties can have a minimal influence on interpretation.

What can cause a baby to be small?
A baby is called small if it is within the smallest 10 percent of babies. If a baby is small, it may be just naturally small, or there could be another reason. The placenta might not be working well, or it could be due to a syndrome, a virus, a disease in the mother, smoking, anemia or poor nutrition.
Diagnosing the cause is not always easy. Your doctor will evaluate all possibilities to determine the most likely cause. There is usually not one tool that gives a clear answer right away. Instead, doctors look at patterns by checking all signs. Each situation needs its own approach.
Read more
Causes of smallness can be:
- Constitutionally small: this means that the baby is naturally small because of their genetics. It’s not due to health problems, but it is just how they are built. Among all small babies, this is the most common reason. But it can only be concluded after excluding other causes.
Health problems
- Placenta: mostly indicated if the blood flow between the mother and baby is abnormal or if the baby’s growth trajectory is abnormal.
- Syndrome-related problem: if the baby is small for gestational age, this should also be considered. Tests to assess this are an anomaly scan (20-week ultrasound), non-invasive prenatal testing (NIPT) or amniocentesis.
- Viral infection: some viruses, like cytomegalovirus or parvovirus, can cause abnormal growth. Recent infections can be tested in the mother’s blood.
- Disease of the mother: some diseases of the mother can affect blood flow to the womb. Examples are diabetes and high blood pressure.
- Anemia: severe and prolonged anemia can affect the transport of oxygen to the womb.
Environmental factors
- Smoking: if a pregnant woman smokes, it can cause low oxygen levels for the baby.
- Malnourishment: if a pregnant woman has severe dietary deficiencies, it can affect the baby’s growth.
How to find a baby with abnormal growth because of a poor functioning placenta?
To check the growth of the baby, we compare the baby’s size to normal values. The challenge is to find the baby who is not growing well because the placenta is not working properly. This is more likely at the lowest percentiles or if there is a drop in the percentiles in subsequent measurements during the pregnancy. We also look for abnormalities in the blood flow in the baby’s umbilical cord and brain, or in the mother’s blood vessels that supply the womb. If the baby is relatively small and the blood flow in the baby and the mother are abnormal, this can be a sign of a poor functioning placenta.
Read more
Blood vessels are assessed with Doppler ultrasound. It shows the blood flow velocity patterns and the measurements reflect the resistance of the organs that the blood is flowing to. Each vessel has its own normal pattern.
The blood vessels that are most often measured are:
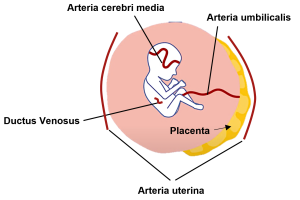
- Arteria uterina (uterine artery): the blood vessel of the mother that supplies blood to the womb. An abnormal measurement can indicate that the placental development has not been optimal.
- Arteria umbilicalis (umbilical artery): the artery in the umbilical cord. An abnormal measurement may suggest high resistance in the placenta, which may be simplified as ‘the placenta is too small for this baby’. This measurement reflects the increased effort from the heart of the baby.
- Arteria cerebri media (middle cerebral artery): this is an important blood vessel in the brain of the baby. If the placenta does not work well, the baby redistributes blood, sends more blood towards the most important organs (the brain and the heart). This is a good compensation because it helps the organs that are most important for survival, but it also means that there is a problem.
- Ductus venosus: this is the blood vessel that transports the oxygen-rich blood from the placenta back to the heart of the baby. When the baby’s heart is struggling to perform the increased effort and starts to fail, this may be seen here.
Why is it important to find FGR early?
Diagnosing FGR early is very important. If the placenta does not work well, it can cause health problems for the baby and sometimes also for the mother. At the end-stage, low oxygen levels can be very dangerous for the baby.
There is no treatment or medication currently available to improve the function of the placenta or the growth of the baby. However, if we know there is an increased risk of low oxygen levels, a plan can be made to monitor the baby and mother closely during further pregnancy. Sometimes this can be done from home with outpatient appointments, or the mother may need to be admitted to the hospital. Ways to monitor include doing ultrasounds to check the blood flow and growth of the baby and regularly performing cardiotocography (CTG). This way, if there is a high risk of low oxygen levels, quick action can be taken, and the baby can be born.
Read more
The CTG is a test used during pregnancy to monitor the baby’s heartbeat and the mother’s contractions. It helps doctors check the baby’s well-being and detect any signs of distress. The test is usually done in the hospital, but sometimes it can be done at home. The information is recorded on a graph on a monitor, which doctors can analyze to see how the baby is doing.
What are the consequences and risks of FGR for the baby?
Please remember that every situation is different and has its own approach and outcomes. In general, there are risks related to FGR, but the risks are depending on how severe the signs and symptoms are.
Several factors are very important for understanding the risks:
- Gestational age at birth
- The further along the pregnancy is at birth, the better the chances of avoiding serious complications. This is the most important factor.
- Severity of growth restriction
- The more the growth is affected, the higher the risk of problems after birth.
- The baby’s condition at birth.
- If the baby, in addition to being too young and too small, also has a serious oxygen problem around birth, this can lead to serious complications.
Before birth
If the baby is at an acceptable gestational age and estimated weight, doctors will carefully check its condition frequently. One of the risks of FGR is stillbirth, which can occur if the oxygen problem gets worse. That is why it is important to monitor the baby. If there are signs of low oxygen levels or that the baby is not doing well, the doctors will need to have the baby born in time to prevent stillbirth. This is usually done through a caesarean section (c-section).
Read more
After birth
Immediately after birth, a pediatrician will check your baby. Depending on the condition, the baby might need some extra help, such as help with breathing or an intravenous line. The baby may need to go to the NICU (a special care unit for newborns) for further support.
Premature babies need help with many body functions in the first weeks after birth because these take time to fully develop. That is why the baby will stay in an incubator until it is old and big enough. This can take several weeks or months. Usually, we recommend that babies stay in the hospital until their due date if everything goes well. After leaving the hospital, it is very important to have regular check-ups to monitor your baby’s development over time.
Over the next days, weeks, and months, doctors will monitor and support all the baby’s important organs systems. Here are some examples:
- Lungs
- Some babies need help with breathing. The baby might only need a little help with airflow through their nose while they are essentially breathing on their own. In more serious cases, they might need a mask or a tube to completely support the baby’s breathing.
- Gut
- In severe early-onset FGR, it may take a long time for the baby’s gut to allow full feedings. At first, the baby may be fed through a tube into their stomach. They may also need extra feeding through the intravenous line until their gut is ready. Pumped breast milk is preferred for feeding when possible.
- Brain
- Premature babies with FGR have a higher risk of brain bleeds. These are different from bleeds in adults, but can lead to problems with brain development.
- Immune system
- The baby is at a high risk of infection. Therefore, there are strategies to prevent them and to use antibiotics when needed.
Most babies born with early-onset FGR will catch up in growth. By the age of 2-3 years, many will reach a size that is normal for their age, taking into account their early birth.
Some children will have problems with neurological development, which may vary in severity (mild or severe). These problems may affect movement (motor skills) or thinking and learning (cognitive skills), and in severe cases, they can have an impact on the quality of life. However, it is hard to generalize these risks. The risks depend on how far along the pregnancy was at the time of birth, the indication of birth, and whether there were complications during pregnancy, childbirth, or afterward. Many babies grow up healthy or with only minor problems.

Other questions
See our FAQ